The hip arthroscopy uses small incisions and special tools to treat certain diseases and conditions of the hip.
The most common hip conditions treated with arthroscopy include labral pathology, femoro-acetabular impingement (FAI) and ligament issues.
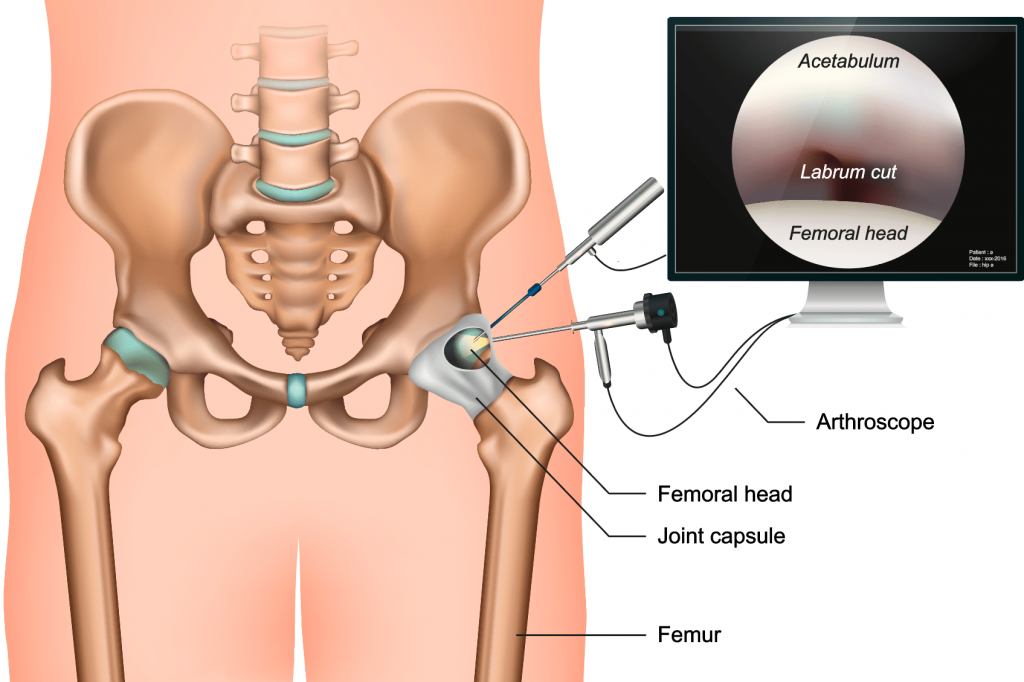
Hip arthroscopy is a surgical procedure that allows doctors to view the hip joint without making a large incision (cut) through the skin and other soft tissues. Arthroscopy is used to diagnose and treat a wide range of hip problems.
During hip arthroscopy, your surgeon inserts a small camera, called an arthroscope, into your hip joint. The camera displays pictures on a video monitor, and your surgeon uses these images to guide miniature surgical instruments.
Because the arthroscope and surgical instruments are thin, your surgeon can use very small incisions, rather than the larger incision needed for open surgery. This results in less pain for patients, less joint stiffness, and often shortens the time it takes to recover and return to regular activities.
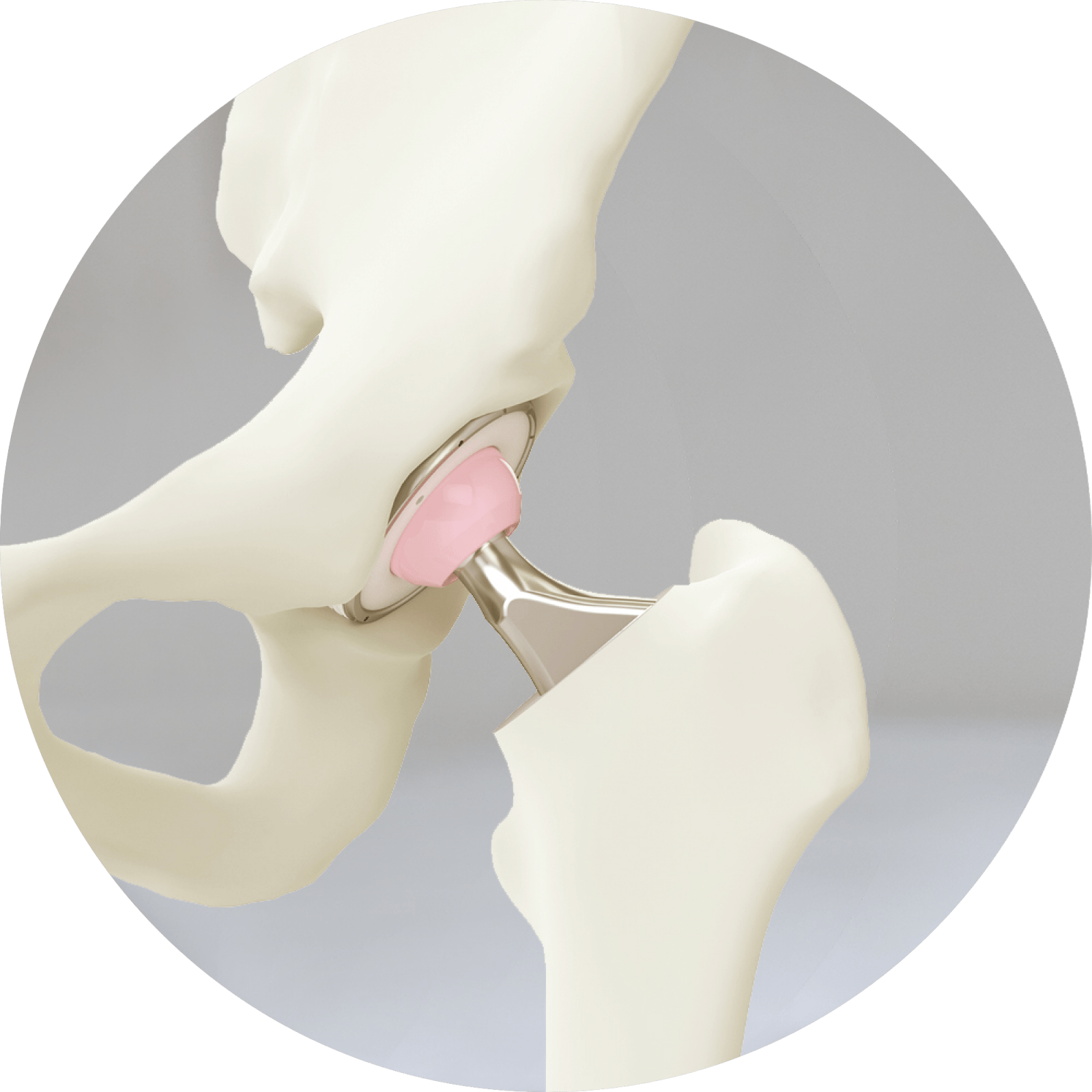
Anatomy
The hip is a ball-and-socket joint. The socket is formed by the acetabulum, which is part of the large pelvis bone. The ball is the femoral head, which is the upper end of the femur (thighbone).
A slippery tissue called articular cartilage covers the surface of the ball and the socket. It creates a smooth, frictionless surface that helps the bones glide easily across each other.
The acetabulum is ringed by strong fibrocartilage called the labrum. The labrum forms a gasket around the socket.
The joint is surrounded by bands of tissue called ligaments. They form a capsule that holds the joint together. The undersurface of the capsule is lined by a thin membrane called the synovium. It produces synovial fluid that lubricates the hip joint.
When Hip Arthroscopy Is Recommended?
Your doctor may recommend hip arthroscopy if you have a painful condition that does not respond to nonsurgical treatment. Nonsurgical treatment includes rest, physical therapy, and medications or injections that can reduce inflammation.
Hip arthroscopy may relieve painful symptoms of many problems that damage the labrum, articular cartilage, or other soft tissues surrounding the joint.
Although this damage can result from an injury, other orthopaedic conditions can lead to these problems, including:
- Femoroacetabular impingement (FAI) is a disorder in which extra bone develops along the acetabulum (pincer impingement) or on the femoral head (cam impingement). This bone overgrowth—called spurs—damages the soft tissues of the hip during movement. Sometimes bone spurs develop in both the acetabulum and femoral head.
- Dysplasia is a condition in which the hip socket is abnormally shallow. This puts more stress on the labrum to keep the femoral head within the socket, and makes the labrum more susceptible to tearing.
- Snapping hip syndromes cause a tendon to rub across the outside of the joint. This type of snapping or popping is often harmless and does not need treatment. In some cases, however, the tendon is damaged from the repeated rubbing.
- Synovitis causes the tissues that surround the joint to become inflamed.
- Loose bodies are fragments of bone or cartilage that become loose and move around within the joint.
- Hip joint infection
Complications
Complications from hip arthroscopy are uncommon. Any surgery in the hip joint carries a small risk of injury to the surrounding nerves or blood vessels, or the joint itself. The traction needed for the procedure can stretch nerves and cause numbness, but this is usually temporary.
There are also small risks of infection, as well as blood clots forming in the legs (deep vein thrombosis).
Recovery
After surgery, you will stay in the recovery room for 1 to 2 hours before being discharged home. You will need someone to drive you home and stay with you at least the first night. You can also expect to be on crutches, or a walker, for some period of time.
-
Pain Management
After surgery, you will feel some pain. This is a natural part of the healing process. Your doctor and nurses will work to reduce your pain, which can help you recover from surgery faster. Medications are often prescribed for short-term pain relief after surgery. Many types of medicines are available to help manage pain, including opioids, non-steroidal anti-inflammatory drugs (NSAIDs), and local anaesthetics. A combination of these medications may improve pain relief, as well as minimise the need for opioids.
Be aware that although opioids help relieve pain after surgery, they are a narcotic and can be addictive. It is important to use opioids only as directed by your doctor. As soon as your pain begins to improve, stop taking opioids. Talk to the orthopaedic team if your pain has not begun to improve within a few days of your surgery.
-
Medications
In addition to medicines for pain relief, you may also be recommended medication such as aspirin, clexane or Xarelto to lessen the risk of blood clots.
-
Swelling
Keep your leg elevated as much as possible for the first few days after surgery. Apply ice as recommended by your doctor to relieve swelling and pain.
-
Dressing Care
You will leave the hospital with a dressing covering your knee. Keep your incisions clean and dry. Instructions will be given which will tell you when you can shower or bathe, and when you should change the dressing (usually 1 week). The orthopaedic team will see you in the office a few days after surgery to check your progress, review the surgical findings, and begin your postoperative treatment program.
-
Bearing Weight
Many patients need crutches or other assistance after arthroscopic surgery. In most cases you will be able to weight bear. If thing differ, Dr Hutabarat will tell you when it is safe to put weight on your foot and leg. If you have any questions about bearing weight, please call the hospital or the rooms.
-
Rehabilitation Exercise
You should exercise your knee regularly for several weeks after surgery. This will restore motion and strengthen the muscles of your leg and knee. Therapeutic exercise will play an important role in how well you recover. A formal physical therapy program may improve your final result.
-
Driving
Dr Hutabarat will discuss with you when you may drive. Typically, patients are able to drive from <1 to 3 weeks after the procedure.
Can't find what you are looking for?
Have a question or inquiry or looking for some more information about our services, get in touch and we will be happy to assist.