Wrist arthroscopy involves keyhole surgery of the wrist.
A fibreoptic telescope attached to a camera is used to visualize inside the wrist joint. A shaver and other tools can be used through another portal for various procedures.

Anatomy
The wrist is a complex joint with eight small bones and many connecting ligaments; a collection of multiple bones and joints.
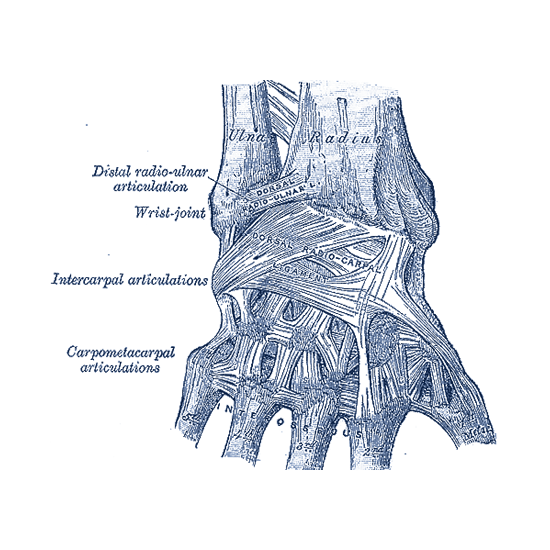
The bones comprising the wrist include the distal ends of the radius and ulna, 8 carpal bones, and the proximal portions of the 5 metacarpal bones.
Arthroscopic surgery can be used to diagnose and treat a number of conditions of the wrist, including chronic wrist pain, wrist fractures, ganglion cysts, and ligament tears.
The Procedure
The surgeon makes small incisions (called portals) through the skin in specific locations around a joint.
These incisions are less than half an inch long. The arthroscope, which is approximately the size of a pencil, is inserted through these incisions. The arthroscope contains a small lens, a miniature camera, and a lighting system.
The three-dimensional images of the joint are projected through the camera onto a television monitor. The surgeon watches the monitor as he or she moves the instrument within the joint.
Probes, forceps, knives, and shavers at the ends of the arthroscope are used to correct problems uncovered by the surgeon.
Diagnostic Arthroscopy
Diagnostic arthroscopy might be used if it is not clear what is causing wrist pain. It might also be used if wrist pain continues for several months despite nonsurgical treatment.
Before arthroscopic surgery, your doctor will do the following.
Perform a physical examination of the hand and wrist
Learn more about past medical conditions or concerns (medical history)
Perform tests that locate the pain (provocative tests). These tests involve moving the hand in order to reproduce the pain.
Secure images of the hand and wrist. These may include x-rays, magnetic resonance imaging (MRI) scans, or an arthrogram (an x-ray taken after a dye is injected into the joint).
Usually, arthroscopic surgery requires only that the hand and arm are numbed (regional anesthesia). A sedative may be given to further relax the patient.
Two or more small incisions (portals) are made on the back of the wrist. The arthroscope and instruments are inserted through those portals and the joint is observed through the camera on the end of the arthroscope.
After the surgery, the incisions are closed with a small stitch and a dressing is applied. Sometimes a splint is used.
Arthroscopic Surgical Treatment
Arthroscopic surgery can be used to treat a number of conditions of the wrist.
- Chronic wrist pain. Arthroscopic exploratory surgery may be used to diagnose the cause of chronic wrist pain when the results of other tests do not provide a clear diagnosis. Often, there may be areas of inflammation, cartilage damage, or other findings after a wrist injury. In some cases, after the diagnosis is made, the condition can be treated arthroscopically as well.
- Wrist fractures. Small fragments of bone may stay within the joint after a bone breaks (fractures). Wrist arthroscopy can remove these fragments, align the broken pieces of bone, and stabilize them by using pins, wires, or screws.
- Ganglion cysts. Ganglion cysts commonly grow from a stalk between two of the wrist bones. During an arthroscopic procedure, the surgeon can remove the stalk, which may reduce the change that these cysts will return.
- Ligament/TFCC tears. Ligaments are fibrous bands of connective tissue that link or hinge bones. They provide stability and support to the joints. The TFCC is a cushioning structure within the wrist. A fall on an outstretched hand can tear ligaments, the TFCC, or both. The result is pain with movement or a clicking sensation. During arthroscopic surgery, the surgeon can repair the tears.
- Carpal tunnel release. Carpal tunnel syndrome is characterized by numbness or tingling in the hand, and sometimes with pain up the arm. It is caused by pressure on a nerve that passes through the carpal tunnel. (The carpal tunnel is formed by the wrist bones and a thick tissue roof.) Pressure can build up within the tunnel for many reasons, including irritation and swelling of the tissue (synovium) that covers the tendons. If the carpal tunnel syndrome does not respond to nonsurgical treatment, one option is to repair the area surgically. The surgeon would cut the ligament roof and enlarge the tunnel. This would reduce pressure on the nerve and relieve symptoms. This can sometimes be done using an arthroscope.
Complications
Complications during or after arthroscopic wrist surgery are unusual. They may include infection, nerve injuries, excessive swelling, bleeding, scarring, or tendon tearing. Your doctor will discuss the complications of arthroscopy with you before your surgery.
Recovery
For the first 2 or 3 days after surgery, the wrist should be elevated and the bandage should be kept clean and dry. Ice may help keep swelling down. There are exercises that can be used to help maintain motion and rebuild your strength. Although pain after surgery is usually mild, analgesic medications will help relieve any pain.
-
Pain Management
After surgery, you will feel some pain. This is a natural part of the healing process. Your doctor and nurses will work to reduce your pain, which can help you recover from surgery faster. Medications are often prescribed for short-term pain relief after surgery. Many types of medicines are available to help manage pain, including opioids, non-steroidal anti-inflammatory drugs (NSAIDs), and local anaesthetics. A combination of these medications may improve pain relief, as well as minimise the need for opioids.
Be aware that although opioids help relieve pain after surgery, they are a narcotic and can be addictive. It is important to use opioids only as directed by your doctor. As soon as your pain begins to improve, stop taking opioids. Talk to the orthopaedic team if your pain has not begun to improve within a few days of your surgery.
-
Medications
In addition to medicines for pain relief, you may also be recommended medication such as aspirin, clexane or Xarelto to lessen the risk of blood clots.
-
Swelling
Keep your leg elevated as much as possible for the first few days after surgery. Apply ice as recommended by your doctor to relieve swelling and pain.
-
Dressing Care
You will leave the hospital with a dressing covering your knee. Keep your incisions clean and dry. Instructions will be given which will tell you when you can shower or bathe, and when you should change the dressing (usually 1 week). The orthopaedic team will see you in the office a few days after surgery to check your progress, review the surgical findings, and begin your postoperative treatment program.
-
Bearing Weight
Many patients need crutches or other assistance after arthroscopic surgery. In most cases you will be able to weight bear. If thing differ, Dr Hutabarat will tell you when it is safe to put weight on your foot and leg. If you have any questions about bearing weight, please call the hospital or the rooms.
-
Rehabilitation Exercise
You should exercise your knee regularly for several weeks after surgery. This will restore motion and strengthen the muscles of your leg and knee. Therapeutic exercise will play an important role in how well you recover. A formal physical therapy program may improve your final result.
-
Driving
Dr Hutabarat will discuss with you when you may drive. Typically, patients are able to drive from <1 to 3 weeks after the procedure.
Frequently Asked Questions
-
How long am I in for?
Just the for part of the day. There is a bit of time waiting around before and after the surgery so allow about 4 hours
-
How much does it cost?
Surgeons charge different fees for many different reasons so it pays to ask around and get other opinions! We do a quote for all our patients. Don’t be afraid to ask questions. We like questions and are happy to answer them.
-
When can I return to sport?
This depends upon the sport, the level of its intensity and the damage in your knee. We want to get you back as soon as we can and will tailor your return to your situation.
-
When can I get it wet? Or swim? Or surf?
Generally wounds need to stay dry for two weeks and then we may give a bit more time as a precaution. Dr Hutabarat has his personal method of an early return to the ocean if it’s pumping. This can be discussed on a case by case basis.
-
What about timing for my holidays/travel?
This is a very important question! Its best to allow 3 weeks before a trip… again it depends on the situation.
Can't find what you are looking for?
Have a question or inquiry or looking for some more information about our services, get in touch and we will be happy to assist.